What is an insulin pump?

An insulin pump is a small device worn on the body that delivers insulin continuously, day and night. It mimics how a healthy pancreas releases insulin by providing a steady background dose with the option to give extra doses at mealtimes. Most pumps can be programmed to match your individual insulin needs throughout the day.
It replaces the need for multiple daily insulin injections and helps manage blood glucose more steadily. Learning how insulin pumps work can help you decide whether pump therapy might be right for you.
How do insulin pumps work?
Insulin pumps deliver insulin in small, precise amounts and allow users to adjust dosing for meals and corrections. This ongoing delivery helps maintain more stable glucose levels between meals and overnight, while also allowing users to give additional insulin when needed. Most pumps use rapid‑acting insulin only, delivering it continuously rather than relying on long‑acting insulin injections.1
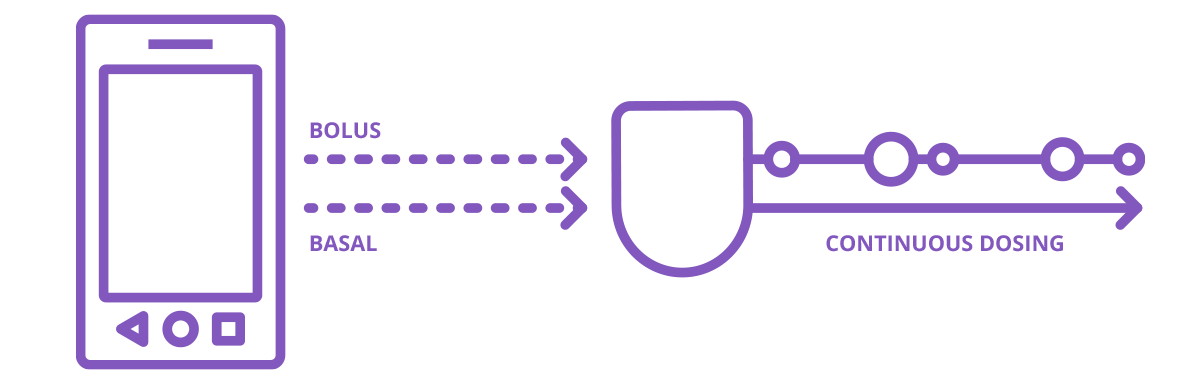
Basal and bolus insulin
Understanding insulin pump therapy starts with two key concepts:
- Basal insulin
Basal insulin, often called background insulin, is delivered steadily throughout the day and replaces the need for long-acting insulin injections.1
- Bolus insulin
Bolus insulin is additional insulin delivered to cover carbohydrates eaten at meals or to correct high blood glucose levels. Bolus doses are given manually using the pump or a controller, depending on the system. Many pumps include built-in bolus calculators to help estimate doses based on personalized settings.1
How insulin pumps deliver insulin
Insulin moves from the pump into your body through an infusion set, which includes:
- Tubing: A thin plastic tube that connects the pump to your body
- Cannula: A small, soft tube placed just under the skin. A needle is used to insert it, then removed, leaving the soft tube in place (often used in tubeless patch pumps)
Insulin pumps and CGM sensors
Insulin pumps can be used alone or alongside a continuous glucose monitor (CGM). A CGM measures glucose levels in real time and shows trends throughout the day and night.
- When worn separately, the CGM provides data and alerts, while the pump continues to deliver insulin based on preset settings.
- In connected systems (often called hybrid closed loop systems or automated insulin delivery systems), the pump and CGM communicate directly. The system automatically adjusts basal insulin delivery based on glucose readings, helping support time in range.
What are the components of an insulin pump?
Insulin pump systems are made up of a few key components that work together to deliver insulin throughout the day. While they all have the same goal, the components differ slightly depending on whether you are using a tubed insulin pump or tubeless (Pod or patch) pump therapy. These components work together to deliver insulin safely and consistently.
What are the different types of insulin pumps?
There are two main categories used in diabetes care today.
Tubed insulin pumps
Also known as tethered pumps, these pumps deliver insulin from a pump worn on clothing or in a pocket. Insulin flows through flexible tubing to an infusion set attached to the body. All controls are typically built into the pump itself.
Tubeless insulin pumps
Also known as patch pumps, these pumps stick directly to the skin with adhesive and deliver insulin without external tubing. The insulin is delivered via a cannula that inserts under the skin. A separate controller wirelessly communicates to the patch pump to administer insulin.
Learn more about Pod therapy with Omnipod
Benefits of using an insulin pump
Many people choose pump therapy because it can offer:
- More precise insulin dosing in very small increments
- Greater flexibility for meals, sleep schedules, and activity
- Reduced need for multiple daily injections
- Support for glucose management when paired with CGM technology1
Who may benefit from an insulin pump
While insulin pumps offer benefits for many people, clinical guidelines help determine who may be eligible for certain technologies. The American Diabetes Association indicates that automated insulin delivery (AID) systems, are preferred over non automated insulin pumps and MDI for those with type 1 diabetes and have largely replaced the use of standard insulin pumps (non-automated).2
For children, adolescents, and adults with type 2 diabetes, the American Diabetes Association recommends automated insulin delivery (AID) systems as the preferred insulin delivery method (over non-automated insulin pumps and MDI).2
Considerations when opting for an insulin pump
While insulin pumps offer many advantages, they may not be the right choice for everyone. Considerations include:
- Wearing a device on the body continuously
- Learning how to program and adjust insulin settings
- Monitoring regularly and changing sites
- Having a back‑up plan in case of pump interruption
Support and structured education from a diabetes care team are essential for safe and effective pump use.
Pod therapy with Omnipod
Pod therapy with Omnipod is a tubeless option designed to simplify insulin delivery without external tubing. Pod systems combine insulin delivery components into a discreet, wearable device and can be part of automated insulin delivery systems when paired with compatible CGM sensors.
Frequently Asked Questions
How do insulin pumps work?
Who should use an insulin pump?
Are insulin pumps used for type 1 diabetes or type 2 diabetes?
What types of insulin pumps are available in the U.S.?

Related Articles



Other topics
References and Disclaimers
1. Cleveland Clinic. Insulin Pumps. Cleveland Clinic. Published December 11, 2023. https://my.clevelandclinic.org/health/articles/insulin-pumps
2. American Diabetes Association Professional Practice Committee; 7. Diabetes Technology: Standards of Care in Diabetes—2026. Diabetes Care 1 January 2026; 49 (Supplement_1): S150–S165. https://doi.org/10.2337/dc26-S007
The Omnipod® 5 Automated Insulin Delivery System is indicated for use by individuals with type 1 diabetes mellitus in persons 2 years of age and older and type 2 diabetes mellitus in persons 18 years of age and older. The Omnipod 5 System is intended for single patient, home use and requires a prescription. The Omnipod 5 System is compatible with the following U-100 insulins: NovoLog®, Humalog®, Admelog®, and Kirsty®.
Refer to the Omnipod 5 Automated Insulin Delivery System User Guide and www.omnipod.com/safety for complete safety information including indications, contraindications, warnings, cautions, and instructions. Warning: DO NOT start to use the Omnipod 5 System or change settings without adequate training and guidance from a healthcare provider. Initiating and adjusting settings incorrectly can result in over-delivery or under-delivery of insulin, which could lead to hypoglycemia or hyperglycemia. WARNING: SmartAdjust technology should NOT be used by anyone under the age of 2 years old. SmartAdjust technology should also NOT be used in people who require less than 5 units of insulin per day as the safety of the technology has not been evaluated in this population.
Available products subject to current insurance coverage and product indication for use. Insulet can only support onboarding for those customers within the product indication.